Author: Mary Francis Grace Marzan
-
Urban Poor Vulnerabilities, Solidarity Networks, and Pathways to Resilience
“Urban Poor Vulnerabilities, Solidarity Networks, and Pathways to Resilience” was presented by Dr. Anna Marie Karaos at the National Resilience Council COVID-19 KNOWLEDGE SERIES Webinar 3 – Resilient Recovery of the Most Vulnerable: Challenges and Opportunities on 12 May 2020. Dr. Karaos’ presentation has been transcribed and the full documentation may be accessed below along…
-
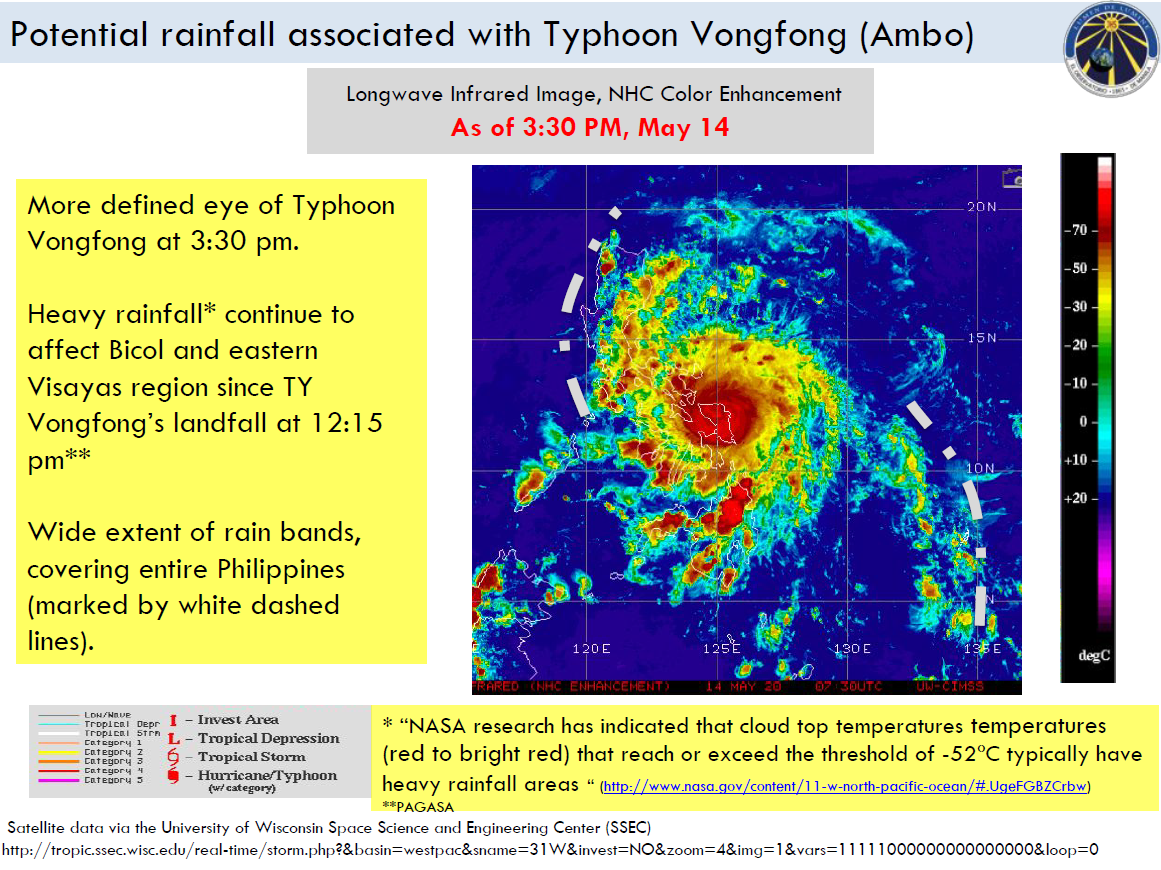
Typhoon Vongfong (Ambo) Report #1
Date: May 14 2020, 6PM PHT | Source: The Manila Observatory Summary WHAT TY Vongfong (Ambo) intensified to Cat 3 (max 1-min sustained winds ~185 kph) and is located over Samar Island (JTWC) as of 14 May 2PM. TY Vongfong made landfall over Eastern Samar on 14 May 12:15PM (PAGASA). WHEN AND WHERE Multi tracks…
-

COVID-19: Opportunities for Resilient Recovery
Date: May 7, 2020 | Source: United Nations Office for Disaster Risk Reduction United Nations Office for Disaster Risk Reduction – Regional Office for Asia and Pacific (UNDRR Asia Pacific) and United Nations Economic and Social Commission for Asia (UNESCAP) and the Pacific International Recovery Platform co-organized a webinar on: COVID-19: Opportunities for Resilient Recovery as…
-
The ultimate vaccine: A resilient health care system
Source: The Philippine Star – Filipino Worldview | Author: Ambassador Roberto R. Romulo | Date: May 8, 2020 Former health secretary Dr. Esperanza Cabral compels us to think beyond today’s crisis. Scientists predict a second wave. The development of a cure and a vaccine for the coronavirus disease 2019 or COVID-19 is going to take time. Even…
-
Quarantine extended
Source: The Philippine Star – Filipino Worldview | Author: Ambassador Roberto R. Romulo | Date: May 1, 2020 President Duterte has extended the enhanced community quarantine to May 15. Despite sentiments of some including LGUs and businessmen, he personally listened to experts, scientists, and former secretaries of health before he agreed with the IATF. In general,…
-

UNDRR ONEA & GETI and WHO Webinar series
Lessons from the COVID-19 pandemic series: Tools for business continuity in the era of COVID-19: How could businesses prepare for reopening? May 7, 2020 | 9:00 PM (GMT +8) Background Up to 80% of all investment in any given country is coming from the private sector. It is there critical that the private sector engages…
-

SMC to donate 560,000 kilos of rice to families under community quarantine
San Miguel Corporation donates 560,000 kilos of rice to various communities throughout Metro Manila as part of its initiative to help mitigate the impact of COVID-19 on millions of families.
-

How South Korea is suppressing COVID-19
Date: March 25, 2020 | Author: Denis McClean | Source: United Nations Office for Disaster Risk Reduction GENEVA, 25 March, 2020 – Trace, test and treat. That sums up the strategy pursued by the Republic of Korea since it detected its first case of COVID-19 on January 20 and its first death on February 20, without…
-

‘Pandemics do not recognise borders, so a united international response is vital under the guidance of WHO’
UNDRR head Mami Mizutori talked with The Times of India about how a comprehensive approach to deal with disasters, backed by international collaboration can be done in the context of the COVID19 outbreak.